
Sonographic Demonstration of Chilaiditi Sign in an Elderly Patient with Respiratory Distress and Abdominal Pain
Dr Himanshu Gul Mirani
Case Presentation:
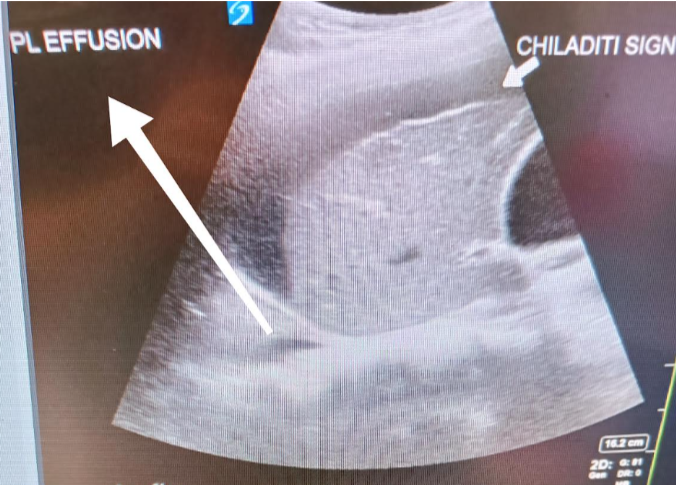
An 80-year-old patient presented with right-sided chest pain, cough, hypoxia requiring supplemental oxygen (1–2 L/min via nasal cannula to maintain SpO₂ >94%), and concurrent right upper abdominal pain, nausea, and vomiting. Point-of-care ultrasound (POCUS) at triage, performed to evaluate the cause of hypoxia, revealed a hypoechoic strip in the subdiaphragmatic region, initially raising suspicion for subphrenic collection. Further scanning demonstrated haustral folds/plicae circularis within the hypoechoic structure, consistent with bowel interposition over the liver. Lung ultrasound revealed right basal consolidation with a small pleural effusion. Chest radiography corroborated the presence of bowel loops between the diaphragm and liver, confirming Chilaiditi sign. Gallbladder assessment showed possible adenomyomatosis, without pericholecystic fluid, shadowing, or mobility with repositioning.
Case History:
Chilaiditi sign is a rare radiological finding in which bowel loops interpose between the liver and right hemidiaphragm. When associated with clinical symptoms, the condition is termed Chilaiditi syndrome. Its significance lies in its potential to mimic more sinister pathologies such as subphrenic abscess, pneumoperitoneum, bowel obstruction, volvulus, or diaphragmatic hernia, often leading to diagnostic uncertainty in acutely unwell patients.
Sonographic Demonstration of Chilaiditi Sign in an Elderly Patient with Respiratory Distress and Abdominal Pain
Management and Outcome:
This is a paragraph. It is connected to a CMS collection through a dataset. Click “Edit Text” to update content from the connected collection.
Key Learnings and Points:
This case highlights the diagnostic challenge posed by Chilaiditi sign, particularly in symptomatic patients where it constitutes Chilaiditi syndrome. The condition may mimic intra-abdominal abscess, pneumoperitoneum, or bowel pathology, with potential for misinterpretation. Sonographic recognition of haustral/plicae markings is a key feature distinguishing bowel interposition from true subdiaphragmatic collections. Awareness of this entity can prevent unnecessary invasive interventions.
Chilaiditi syndrome, although rare, should be considered in elderly patients presenting with respiratory distress and abdominal symptoms. POCUS, when carefully interpreted, can play a critical role in differentiating this benign entity from surgical emergencies, guiding appropriate management and avoiding misdiagnosis.